

IDH1 R132H antibody clone H09 (DIA-H09) is an indispensable tool for Glioma diagnosis with high impact on cancer research as documented by more than 150 scientific publications on CiteAb.
The routine practical approach for diagnosing astrocytomas and oligodendrogliomas begins with perfoming IHC for ATRX and IDH1 R132H expression. Stepwise analysis of molecular parameters with initial IHC for ATRX and IDH1 R132H followed by 1p/19q analysis and then by IDH sequencing significantly reduces the number of molecular tests required for unequivocal diagnosis (Reus et al., Acta Neuropathol. 129, 2015).
Characteristics of the 3 most important molecular groups of adult glioma:
| Diffuse glioma with IDH mutation and 1p/19q-codeletion | Diffuse glioma with IDH mutation | Diffuse glioma without IDH mutation | |
| Biomarker | |||
| IDH1/2 1p/19q ATRX hTERT-Promotor | mutated co-deleted nuclear expression mutated | mutated intact loss of nuclear expression wildtype | wildtype intact nuclear expression mutated |
| Typical histological finding and prognosis | |||
| Histology WHO grading Median Survival | oligodendroglial II oder III >15 years | astrocytic II or III (IV) 8-12 years | astrocytic IV (II or III) <2-3 years |
Moreover, the WHO-classification for CNS Tumors 2016 recommends the analysis of new molecular markers on formalin-fixed tissues and puts a strong focus on the immunohistochemical determination of the IDH1, ATRX and H3-K27M mutation status.
Combined IHC on IDH1 R132H (clone H09) and ATRX (clone AX1) substitutes molecular testing.
IDH1 R132H The 2016 CNS WHO certification recommends IDH1 R132H IHC as a backbone for differential diagnosis of glioma. IDH1 R132H IHC is widely applied as a favorable prognostic marker.
The 2016 CNS WHO certification recommends IDH1 R132H IHC as a backbone for differential diagnosis of glioma. IDH1 R132H IHC is widely applied as a favorable prognostic marker.
ATRX ATRX mutations in gliomas result in the loss of nuclear ATRX expression (right), which can be diagnosed by IHC analysis. Loss of ATRX expression is close to being mutually exclusive to 1p/19q co-deletion.
ATRX mutations in gliomas result in the loss of nuclear ATRX expression (right), which can be diagnosed by IHC analysis. Loss of ATRX expression is close to being mutually exclusive to 1p/19q co-deletion.
IHC detection of somatic H3 K27M mutations defines midline glioma as an independant entity.
Histone H3 K27M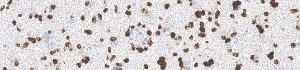 The WHO classification 2016 describes the diffuse midline glioma with H3-K27M mutation as a new entity. It is most common in children and adolescents and is localized in midline structures.
The WHO classification 2016 describes the diffuse midline glioma with H3-K27M mutation as a new entity. It is most common in children and adolescents and is localized in midline structures.
Ki67 and p53 are helpful accessory marker for classification of diffuse glioma.
Ki67 High Ki-67 is dominant in IDH wild type gliomas and low Ki-67 is associaterd with IDH1 mutation in primary glioblastomas. The mitotic index is significantly associated with outcome of IDH wild type tumors.
High Ki-67 is dominant in IDH wild type gliomas and low Ki-67 is associaterd with IDH1 mutation in primary glioblastomas. The mitotic index is significantly associated with outcome of IDH wild type tumors.
p53 p53 can be selected as a marker since there is evidence of relationships among p53, mutually exclusive to 1p/19q deletion, suggesting the usesfulness of ATRX and p53 IHC without 1p/19q analysis.
p53 can be selected as a marker since there is evidence of relationships among p53, mutually exclusive to 1p/19q deletion, suggesting the usesfulness of ATRX and p53 IHC without 1p/19q analysis.
Reference:
Reuss DE et al. ATRX and IDH1-R132H immunohistochemistry with subsequent copy number analysis and IDH sequencing as a basis for an “integrated” diagnostic approach for adult astrocytoma, oligodendroglioma and glioblastoma. Acta Neuropathol. 129(1):133-146, 2015
Reuss DE et al. ATRX and IDH1-R132H immunohistochemistry with subsequent copy number analysis and IDH sequencing as a basis for an “integrated” diagnostic approach for adult astrocytoma, oligodendroglioma and glioblastoma. Acta Neuropathol. 129(1):133-146, 2015